doh-hfsrb-qop-01-form1|DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1 : Bacolod DOH-HFSRB-QOP-01 Form Rev:0 2 6/ 17 / Page 1 of 2 Name of Health Facility (HF) or Service Provider : HF Complete Address : No. & Street Barangay District .
Registration No.: 0396821 MEGA WELL LIMITED is a live company incorporated on 31 December 1992 (Thursday) in Hong Kong as a private company limited by shares entity. This private company limited .businessclub.ihg.com Rent Meeting Rooms, Conference Venues & Training Room Hire Related searches: Ihg Microsoft Outlook , Ihg Outlook , mail Ihg Outlook , Ihg Outlook mail Access , Ihg Outlook mail , Ihg Outlook 365 mail , Ihg mail Outlook Access , Ihg Mail Outlook
PH0 · Revised Application Form DOH
PH1 · PROCESS FLOW OF RENEWAL APPLICATION FOR HEALTH FACILITIES
PH2 · DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1
PH3 · DOH
To refute and to confute are to answer so as to admit of no reply. To refute a statement is to demonstrate its falsity by argument or countervailing proof; confute is substantially the same in meaning, tho differing in usage.Refute applies either to arguments and opinions or to accusations; confute is not applied to accusations and charges, but to arguments or .
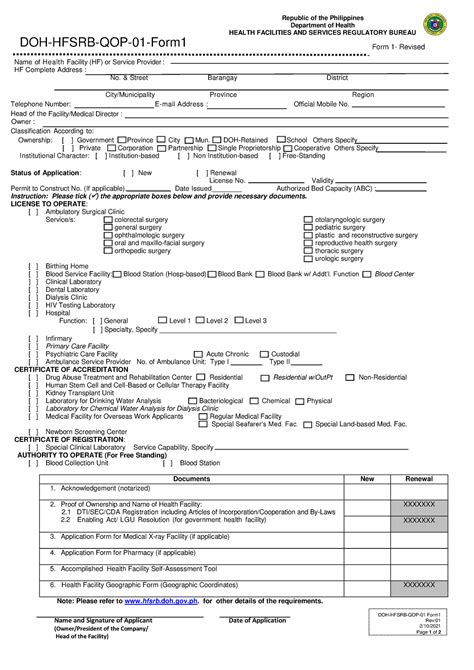
doh-hfsrb-qop-01-form1*******HEALTH FACILITIES AND SERVICES REGULATORY BUREAU. DOH-HFSRB-QOP-01-Form1. Form 1- Revised. Name. of Health Facility (HF) or Service Provider: HF .
HFSRB | Pag Lisensyado. ProtektaDOHdownloading DOH-HFSRB-QOP-01-Form1 Revision 01 (Application for License to .
DOH-HFSRB-QOP-01-Form 2. a. Name HF Complete Address: of Health Facility .HFSRB | Pag Lisensyado. ProtektaDOH - hfsrb.doh.gov.ph
DOH-HFSRB-QOP-01 Form Rev:0 2 6/ 17 / Page 1 of 2 Name of Health Facility (HF) or Service Provider : HF Complete Address : No. & Street Barangay District .
DOH-HFSRB-QOP01Form1 rev2 6172022 - Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free.
Revised Application Form DOH-HFSRB-QOP-01 Form1 | PDF | Surgery | Hospital. Revised Application Form DOH-HFSRB-QOP-01 Form1 - Free download as Word Doc (.doc), .Department of Health. HEALTH FACILITIES AND SERVICES REGULATORY BUREAU. DOH-HFSRB-QOP-01-Form1. Name of Health Facility (HF) or Service Provider : HF .DOH-HFSRB-QOP-01-Form1-3212019-postedDOH-1-1-1.doc - Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free.DOH-HFSRB-QOP01Form1 rev2 6172022 - Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free.
Revised Application Form DOH-HFSRB-QOP-01 Form1 - Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free.
Name and Signature of Applicant Date of Application XXXXXXX DOH-HFSRB-QOP-01 Form1 Rev:00 3/1/2019 Page 1 of 2 Acknowledgement REPUBLIC OF THE PHILIPPINES MUNICIPALITY OF I, ) CITY/ ) S.S. , Name , of legal age, Civil Status , a resident of Age , after having been sworn in accordance with law Address hereby depose and say that I .
DOH-HFSRB-QOP-01 Form1 Rev:00 3/1/2019 Date of Application Eentastsststtnerssuntssnstst Page : 1 of 2: Acknowledgement REPUBLIC OF THE PHILIPPINES MUNICIPALITY OF I, —) CITY/ )S.S. , : Civil Name Of legal age, , Status , resident of a Age after having been sworn in accordance with law Address hereby .DOH-HFSRB-QOP-01 Form Rev:0 2 6/ 17 / Page 1 of 2 Name of Health Facility (HF) or Service Provider : HF Complete Address : No. & Street Barangay District City/Municipality Province Region Telephone Number: E-mail Address : Official Mobile No. Head of the Facility/Medical Director : Owner : Classification According to: Ownership : [ .HFSRB | Pag Lisensyado. ProtektaDOH - hfsrb.doh.gov.phDOH-HFSRB-QOP-01-Form1 . Name and Signature of Applicant. Date of Application. DOH-HFSRB-QOP-01 Form1. Rev:00. 3/1/2019. Title \376\377\000A\000p\000p\000l\000i\000c\000a\000t\000i\000o\000n\000 \000-\000 \000W\000a\000t\000e\000r\000 \000A\000n\000a\000l\000y\000s\000i\000s AuthorDOH-HFSRB-QOP-01 Form1 Rev:02 6/17/2022 Page 2of Acknowledgement REPUBLIC OF THE PHILIPPINES ) CITY/ MUNICIPALITY OF ) S.S. I, , , of legal age, , a resident of Name C iv l S ta us Age _____, after having been sworn in accordance with law Address hereby depose and say that I am executing this affidavit to attest to the completeness .
doh-hfsrb-qop-01-form1 DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1 DOH-HFSRB-QOP-01-Form1 Form 1- Revised DOH-HFSRB-QOP-01 Form Rev: 2/10/ Page 2 of 2 Acknowledgement REPUBLIC OF THE PHILIPPINES ) CITY/ MUNICIPALITY OF ) S. I, , , of legal age, , a resident of Name Civil Status Age _____, after having been sworn in accordance with law Address hereby depose and say that I am .Citation preview. Republic of the Philippines Department of Health HEALTH FACILITIES AND SERVICES REGULATORY BUREAU DOH-HFSRB-QOP-01-Form 2 a Date: Name of Health Facility (HF)/Service Provider HF Address : No. & Street District Barangay City/Municipality Region HF Landline No. Owner Mobile No. Latest LTO/COA/ATO No. .DOH-HFSRB-QOP-01-Form 2 Rev.:02 6/17/2022 Page 1 of 1 Print Name and Signature Name of Health Facility (HF)/Service Provider HF Complete Address: No. & Street Barangay District
DOH-HFSRB-QOP-01-Form1-3212019-postedDOH-1-1-1.doc - Free download as Word Doc (.doc), PDF File (.pdf), Text File (.txt) or read online for free. Scribd is the world's largest social reading and publishing site. .DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1 DOH-HFSRB-QOP-01 Form 3 Rev:00 6/9/2020 Acknowledgement REPUBLIC OF THE PHILIPPINES) CITY/MUNICIPALITY OF _____)S.S. I, _____, _____, of legal age, _____, a resident of Name Civil Status Age .
DOH-HFSRB-QOP-01 Form1 Rev:01 2/10/2021 Page 2 of 2 Acknowledgement REPUBLIC OF THE PHILIPPINES ) CITY/ MUNICIPALITY OF ) S.S. I, , , of legal age, , a resident of Name C iv l S ta us Age _____, after having been sworn in accordance with law Address hereby depose and say that I am executing this affidavit to attest to the completeness .doh-hfsrb-qop-01-form1Get and add pdfFiller Google Chrome Extension to your browser to edit, fill out and eSign your doh hfsrb qop 01 form1, which you can open in the editor directly from a Google search page in just one click. Execute your fillable documents from any internet-connected device without leaving Chrome.Title Application - Water Analysis Author \376\377\000S\000D\000D\000-\000B\000H\000F\000S Created Date: 6/17/2022 4:35:14 PM12/28/2021. Department Memorandum No. 2021-0545 – Decentralization of Licensing and Regulatory Functions for Level 2 General Hospitals from Health Facilities and Services Regulatory Bureau (HFSRB) to the Center for Health Development Regulation, Licensing and Enforcement Division (CHD-RLEDs) 12/24/2021.DOH-HFSRB-QOP-01-Form 2 Rev.:02 6/17/2022 Page 1 of 1 Print Name and Signature Name of Health Facility (HF)/Service Provider HF Complete Address: No. & Street Barangay District
Lawyer native to Marbella with a strong family background from real estate on the Costa del Sol. Experience from several international law firms, focusing on property law, corporate advisory and private law. Holds German & Spanish dual citizenship. Dual legal & business administration degree from University of Granada.
doh-hfsrb-qop-01-form1|DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1